I have had several people ask me what is the difference between all the surgeries? And why did I chose the Route Y one for myself? Here is a breakdown of each of the surgeries that are available to obese patients.
Route Y Bypass (most common):
 |
| Route Y Bypass |
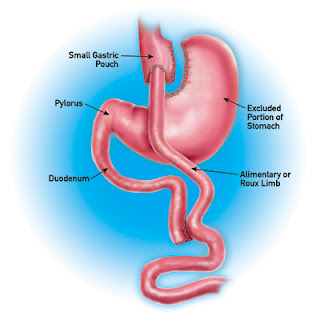
The Roux-en-Y Gastric Bypass is generally considered to be the best surgical procedure for the treatment of morbid obesity. Weight loss is achieved by reducing the functional portion of the stomach to a pouch one ounce or less in size, and by creating a stoma, a small opening between the stomach and the intestine.
The small size of the stomach pouch causes the patient to have a sensation of fullness after eating only a small portion of food. The small stoma delays stomach emptying, making the sensation of fullness last longer. These are called the Restrictive components of the procedure.
The limb of intestine coming down from the small pouch is called the Roux limb. The limb of intestine coming down from the bypassed portion of the stomach can be called the Biliary or Bypassed limb. The remaining portion of the intestine is called the Common Channel. Food does not pass down the Bypassed limb, only the Roux limb and the Common Channel. The longer the Bypassed limb, the less the length of intestine actively working to absorb nutrients from the food that is eaten. Digestive juices that normally help absorb nutrients from the food enter the Bypassed limb from the larger portion of the stomach, the liver, and the pancreas, and pass down the Bypassed limb to the Common Channel. These juices do not mix with the food while it is passing down the Roux limb. The longer the Roux limb, the longer the portion of intestine trying to absorb nutrients without the benefit of these digestive juices. Both of these changes result in less absorption of nutrients and contribute to weight loss, and are called the Malabsorptive components of the procedure.
Exactly how the operation is done for an individual patient depends on their individual anatomy, their general health status, whatever changes they may have from prior surgeries, and what they hope to achieve from the operation. The stomach compartments can be completely divided from each other or simply partitioned, the small stomach pouch and the intestinal limbs may be connected to each other with either staples or sutures, a small band may be placed around the stomach pouch, and the two intestinal limbs may be made longer or shorter. The drawing below depicts the Roux-en-Y Gastric Bypass operation. Note that the two portions of the stomach are completely divided from each other. This is my preferred way of making the pouch, as simply partitioning the stomach instead of completely dividing it may entail a higher risk of the two parts connecting themselves back together, which would defeat the operation. Some very fine surgeons prefer to just partition the stomach and not to divide it completely, and I may choose to do the operation that way from time to time.
My preferred length for each of the intestinal limbs is approximately 100 cm, or 3 feet. These are reasonable lengths of intestine to bypass from the food stream and to isolate from the flow of digestive juices, but still leaves enough (approximately 14 feet) intestine in the Common Channel to allow for adequate nutritional intake. Making the limbs longer will increase the amount of malabsorption, and increase the potential weight loss. But increasing the length of the limbs also increases the requirement for dietary supplementation of vitamins, minerals and protein, increases the incidence of side effects such as diarrhea, and increases the potential for excessive weight loss.
***This information is from my Doctor's website and should always be consulted with your own Bariatric doctor.
Gastric Sleeve Bypass:
 |
| Gastric "Sleeve" Bypass |
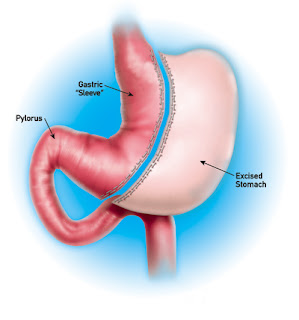
Gastric sleeve surgery (sleeve gastrectomy) is one of the newer forms of bariatric surgery but has quickly been gaining popularity over the recent years. Also known as vertical sleeve gastrectomy, vertical gastroplasty or sleeve gastroplasty, this procedure is another option for those looking to help with their morbid obesity through gastric bypass surgery. The gastric sleeve is a restrictive procedure meaning that it achieves weight loss results by restricting the amount of food that your body is physically able to take in. There is no malabsorption involved with this procedure but can be followed up with a malabsorptive procedure afterwards if the patient wishes.
Gastric sleeve surgery involves permanently removing a large portion of the stomach, anywhere from 60% to 85% of the total stomach. The portion left behind is a slim tube or "sleeve" that will serve as your new stomach. This stomach is already connected naturally to the stomach inlet and outlet which means that no rerouting of the intestines is needed.
What differentiates a gastric sleeve procedure from other weight loss surgeries is the nerves to the stomach and the outlet valve (pylorus) of the stomach remain intact to preserve the functions of the stomach while at the same time, reducing the volume it is able to hold. There is no bypass of the intestines with the gastric sleeve, only stomach capacity reduction. A sleeve gastrectomy also works because it removes the part of the stomach that produces Ghrelin, which is a hormone that stimulates appetite. This helps to noticeably reduce without completely eliminating a person appetite.
Advantages of the Gastric Sleeve
The primary features of gastric sleeve surgery are reducing the size of the stomach up to 85%, to restrict food intake while also reducing the hormones that create the craving for food due to the removal of the excess stomach portion. This reduces the production of the Ghrelin hormone which in turn reduces the hunger sensation.
The advantage of gastric sleeve surgery include:
- 30 to 60% extra weight loss within the first 12 months of the procedure
- Less invasive than gastric bypass
- No cutting or, disconnection or alteration of the intestines
- No risk of “dumping syndrome” typically associated with gastric bypass
- No need for implementation of foreign devices in to the body such as a gastric band
- Less restrictive post-surgery diet
- Procedure may be followed by gastric bypass or duodenal switch for even better results for super obese patients (those with a BMI > 70)
- Can be performed laparoscopically on extremely obese patients
Disadvantages of the Gastric Sleeve
As with any medical procedure of this nature, there is always the potential for adverse affects. The biggest potential drawback for some people with this procedure is that is irreversible and thus you must really understand all of the implications before proceeding with gastric sleeve surgery.
In addition the following potential drawbacks should be taken in to consideration:
- Since the gastric sleeve is a restrictive weight loss procedure and not malabsorptive, inadequate weight loss or weight regain is more likely to occur than would in a procedure involving intestinal bypass
- The newly created pouch has the potential to stretch over time
- Weight Loss only really noticeable with total change in diet combined with exercise
- Additional surgery may be required for follow-up procedures to combine methods
- Leakage may occur at the site of stapling
- Still no knowledge of long term results due to short history of procedure
- Insurance may not cover due to the short history of the procedure making the cost potentially prohibitive for many people
- Advantages of the Gastric Sleeve
- The primary features of gastric sleeve surgery are reducing the size of the stomach up to 85%, to restrict food intake while also reducing the hormones that create the craving for food due to the removal of the excess stomach portion. This reduces the production of the Ghrelin hormone which in turn reduces the hunger sensation.
- The advantage of gastric sleeve surgery include:
- 30 to 60% extra weight loss within the first 12 months of the procedure
- Less invasive than gastric bypass
- No cutting or, disconnection or alteration of the intestines
- No risk of “dumping syndrome” typically associated with gastric bypass
- No need for implementation of foreign devices in to the body such as a gastric band
- Less restrictive post-surgery diet
- Procedure may be followed by gastric bypass or duodenal switch for even better results for super obese patients (those with a BMI > 70)
- Can be performed laparoscopically on extremely obese patients
- Disadvantages of the Gastric Sleeve
- As with any medical procedure of this nature, there is always the potential for adverse affects. The biggest potential drawback for some people with this procedure is that is irreversible and thus you must really understand all of the implications before proceeding with gastric sleeve surgery.
- In addition the following potential drawbacks should be taken in to consideration:
- Since the gastric sleeve is a restrictive weight loss procedure and not malabsorptive, inadequate weight loss or weight regain is more likely to occur than would in a procedure involving intestinal bypass
- The newly created pouch has the potential to stretch over time
- Weight Loss only really noticeable with total change in diet combined with exercise
- Additional surgery may be required for follow-up procedures to combine methods
- Leakage may occur at the site of stapling
- Still no knowledge of long term results due to short history of procedure
- Insurance may not cover due to the short history of the procedure making the cost potentially prohibitive for many people.
Duodenal Switch
Duodenal switch is a bariatric surgical procedure employed to combat obesity. This form of bariatric surgery helps obese patients control their weight and begin the path to a healthier, more active lifestyle. Not all obese individuals qualify for this form of surgery. Good candidates have a body mass index (BMI) of 40 or more. Candidates with a BMI of 35 qualify if they show signs of unhealthy, weight-related symptoms such as heart disease or diabetes.
The surgery consists of a restrictive and malabsorptive surgical procedure. The restrictive element is a partial gastrectomy that reshapes and removes a portion of the stomach. The remaining portion, where the food exits, resembles a banana and has a capacity of around six ounces.
The malabsorptive element separates the flow of bile and pancreatic juices by rearranging the small intestines. Further down, the physician reconnects the two intestinal paths. The food and digestive juices combine in the last 18 to 24 inches of the small intestine. Limited fat absorption takes place as the food heads towards the large intestine.
Advantages of Duodenal Switch
People who choose duodenal switch surgery experience greater weight loss with a low risk of weight gain. The pyloric valve, the portion of the stomach connected to the duodenum, remains intact. As a result, patients do not experience the “dumping” syndrome commonly associated with the Roux-en-Y Gastric Bypass. The malabsorptive component is partially reversible for patients with malabsorption difficulties. Duodenal switch patients experience weight loss at a more rapid pace compared to those who choose the laparoscopic banding procedure. In addition the following are all potential advantages of the Duodenal Switch procedure:
- Typically greater weight loss over a longer period of time
- Weight loss of up to 60% to 80%
- Patients can eat a more "normal" and less restrictive diet compared to gastric bypass or gastric banding
- No "dumping syndrome"
- Intestinal rerouting is reversible
- People with very high BMI and extreme obesity who are not eligible for other weight loss surgeries may still qualify for the Duodenal Switch
Disadvantages of Duodenal Switch
Duodenal switch surgery carries more risks compared all other traditional weight loss surgeries. Complications occur more often in this form of surgery due to a higher BMI. Patients may lose too much weight. Duodenal switch patients may experience long-term nutritional deficiencies and be subject to a lifetime of medication and special foods. Other complications include anemia, infection, gallstones and hernias. Other potential disadvantages include:
- Most complex of all the weight loss surgery options
- Certain foods may become intolerable
- Increased risk for intestinal problems or gallstones
- Potential for malnutrition or vitamin deficiency
- Potential for frequent gas, bloating or change in body odor
Risks & Complications
Gastric Banding/Lap Band
(usually recommended only up to 75lbs of loss)
Gastric banding, or laparoscopic adjustable banding is a bariatric surgery procedure that uses an adjustable belt placed around the upper portion of the stomach. This band is made out of silicone and is designed to constrict the size of the stomach and the amount of food that can be held in the stomach. At the same time, it slows down the passage of food to the intestines which helps signal to the brain that the stomach is full. The band is filled with saline which can be increased or decreased based upon your needs and your doctors recommendations. A small port is accessed near the surface of the skin that your doctor can then add or remove saline through. Adding saline tightens the band and shrinks the size of the stomach pouch that can accept food. This should make you feel fuller, quicker and decrease the appetite and as a result help you lose weight.
While gastric banding is meant to be a long term weight loss remedy, some people will require a follow up procedure to re-position, replace or remove the gastric band. This could be due to complications or ineffectiveness of the band.
There are two primary options you can choose from when deciding if a gastric band is the right option for you. The LAP-Band and REALIZE Band are very similar in many ways but there are slight differences between the two. Learn more about how to
choose which band is right for you.
Advantages of Gastric Banding
- With gastric banding you typically have a shorter operation, lasting around 1 hour
- You're in the hospital recovering for no more than 24 hours total. This is compared to a 2-3 hour surgery with gastric bypass and a multiple day stay in the hospital for recovery.
- Total recovery time is reduced to 6 weeks, down from 3 months, when opting for gastric banding.
- Gastric banding is one of the safer weight loss surgeries
- Procedure is reversible
Disadvantages of Gastric Banding
- Patients must work harder to lose weight after this procedure is complete since it relies on food restriction only, and is not a malabsorptive procedure in the way that other bariatric surgery procedures achieve their results.
- This means that your diet will be restricted for a longer period of time after gastric banding.
Complications Related to Gastric Banding
Gastric banding is relatively new when compared with gastric bypass surgery and there are some key differences when you compare the two procedures. The advantages of gastric banding over gastric bypass or other bariatric surgeries are:
There are however, some drawbacks for choosing this procedure.
There are common complications related to gastric banding that affect all types of weight loss surgeries including nausea, vomiting or risk of infection. There are however, also unique
complications related to gastric banding that you should be aware of before deciding on the bariatric surgery that is right for you.
Writer's Note: All these procedures should be talked in-depth with your surgeon/doctor. Your choice is ultimately yours as you will have to live with the results of the surgery. Always use caution and research using multiple outlets for your decision.




